QUOTE(tqeh @ Dec 17 2012, 07:02 PM)
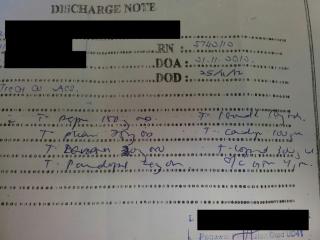
It is likely that it is a unintentional mistake (for aspirin and ?cardiprin).
Not sure why gemfibrozil, does it actually really work? Definitely I wont feel comfortable starting them together.
? consider beta blocker in future?
Statin is a must regardless of lipid studies given its role in secondary prevention.
Plavix - did not state the duration? Was PCI done/ BMS/ DES? =D
Such mistake would not be made if there is a pharmacist around checking discharge scripts?
As mentioned, I hope this is an unintentional mistake. If not then I am very worried about the quality of medical education.
yes, agreed with the statin part. Statin should be started regardless of lipid profile post ACS/STEMI. Like you, I am also not comfortable with starting both fibrate and statin.
if I am not mistaken, PCI is not routinely done for ACS. It is however, a gold standard for STEMI. Also, district hospital has no cardiologist, so PCI can't be done.
Well, I am equally surprised that pharmacist didn't pick up the mistakes.
QUOTE(zstan @ Dec 17 2012, 07:22 PM)
yes but this was a discharge script. the patient might have already been started on initial therapy during admission. no? furthermore it is unclear on how long has the patient been admitted and what other drugs has the patient been taking along with his other test results. IMO besides the duplication of aspirin, its hard to justify whether the script is accurate or not based on present data.
gemfibrozil is to lower TGL levels, beta blockers work on the heart. both drugs work differently and have different mechanisms and different outcomes.

u only start statins if patient has a previous cardio/stroke event. if levels all ok then no issue la. but having said that if you get admitted probably got problem liao.
I guess you are confused a little. Let me clarify.
1. The guideline says optimal monotherapy before considering combination. Does 20mg of lovastatin or 300mg of gemfibrozil sound optimal to you? Are you aware of the max dosage for each drug?
2. Date of admission and discharge clearly written on the discharge note. Pls read it carefully.
3. All drugs taken by the patient are on the discharge note (usual practice for hospitals)
4. You dun only start statin post stroke or cardio event (where did you get this fact!?). Statin can be used in simple dyslipidemia as suggested by KKM guideline and guidelines all over the world.
5. tqeh is right on beta blocker for ACS. Beta blocker reduces the myocardial oxygen demand, thus it benefits patients with ACS/STEMI as well as CCF.
I would suggest you do a read through of KKM's guidelines as well as books such as Sarawak Handbook of Medical Emergencies. Are you a doctor btw? If I am not mistaken, you are a pharmacist right?
Added on December 17, 2012, 8:38 pmQUOTE(onelove89 @ Dec 17 2012, 07:40 PM)
was looking for beta blockers in the chart and trying to make up what is what. to be honest i've never heard of cardiprin, we just say low dose asp 100mg.

but yeah, double prescription seems like an unintentional mistake? (overworked? still, not an excuse).
I'll still put in statins and asp just for prevention, for high risk patients. as far as i know, statins are relatively safe, well, apart from some causing rhabdo, but chances are rather low. and I wouldn't be so sure on prescribing fibrates with statin tgt.
Cardiprin is combination of 100mg aspirin and 45mg glycine. It causes less gastrointestinal effect than conventional aspirin.
This post has been edited by hypermax: Dec 17 2012, 08:38 PM 

 Dec 12 2012, 06:32 PM
Dec 12 2012, 06:32 PM
 Quote
Quote








 price? dosage? compliance?
price? dosage? compliance? 0.0289sec
0.0289sec
 0.52
0.52
 6 queries
6 queries
 GZIP Disabled
GZIP Disabled