



Anyway, I do realize the lack of post grad discussion in this thread. Seems to me not many are keen for further studies

CALLING ALL MEDICAL STUDENTS! V3, medical student chat+info center
|
|
 Dec 11 2012, 11:55 PM Dec 11 2012, 11:55 PM
Return to original view | Post
#1
|
 
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
Wow, version 3 already? There seems to be a lot of info on Australia, guess many interested to practice there eh? Oh no, here comes the brain drain
Anyway, I do realize the lack of post grad discussion in this thread. Seems to me not many are keen for further studies |
|
|
|
|
|
Dec 12 2012, 12:36 AM
Return to original view | Post
#2
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(limeuu @ Dec 12 2012, 12:26 AM) the discussion is about potential and current students in oz, and does not mean necessarily means working there, and there is increasing probability that many will not get internship jobs there in future.... To my knowledge, most people who attend med schools in developed countries do have the intention of working there upon graduation (scholars not included). So anyhow, privately funded medical students studying in developed countries do largely contribute to the brain drain phenomenon.also, this thread is about medical students, hence the focus in about getting into, and focusing on medical studies.....postgraduate issues will be inappropriate for students at this point......  Anyway, no harm discussing about postgrad studies here even though the thread is meant for medical students. Perhaps a senior doc like yourself can start the ball rolling. It would definitely be nice for a senior clinician such as yourself to shed some light on this matter. |
|
|
Dec 12 2012, 01:15 AM
Return to original view | Post
#3
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(limeuu @ Dec 12 2012, 01:02 AM) intentions, and the actual ability to are different matters.....and increasingly, both uk and oz are closing doors to international students staying on and working after graduating..... To my knowledge, uk's door has long been closed for non eu citizens. Imgs can only do foundation years there, and will be required to leave upon completion. As for oz, they are still taking in mos who has completed amc test (some of my classmates just went). Just that the internship post is limited.the same will be happening to working in spore as well, in the near future..... which is why is amusing to read students of local med schools not recognised elsewhere talk about going to work and do postgraduate training in these developed countries.... as for postgraduate issues, pagalavan's blog would probably be a better place to ask and discuss..... Btw are u from Kuching? Do you know anything about cardiology department in Sarawak GH? I heard training under Dr Sim is very good. |
|
|
Dec 12 2012, 01:27 AM
Return to original view | Post
#4
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(limeuu @ Dec 12 2012, 01:21 AM) img refers to doctors who graduated outside these countries.....international students who studied and graduated there are not considered img..... Oh my bad. What I meant was non eu citizens who have completed their studies in uk.it is possible to get jobs beyond fy in uk....the visa requirements will be met, as long as there is a job offer, and that is possible in some circumstances....particularly for top students with good references..... dr. sim is no longer with the moh officially.... So without dr sim, does the cardiology in SGH still offer good training? |
|
|
Dec 17 2012, 11:35 AM
Return to original view | Post
#5
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
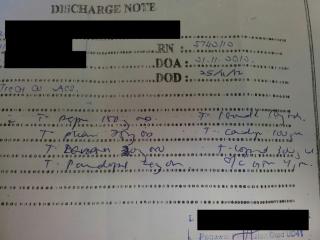
Dear medical students/doctors, pls point out the mistake in this discharge note from a peripheral hospital.
|
|
|
Dec 17 2012, 05:07 PM
Return to original view | Post
#6
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
Yeah, one of the mistakes is the bad hand writing. Doctor's writing supposed to be neat and tidy
This patient was diagnosed with ACS and warded. Upon discharge, he was prescribed the following meds: T. Perindopril 4mg OD T. Aspirin 150mg OD T. Clopidogrel 75mg OD T. Lovastatin 20mg ON C. Gemfibrozil 300mg ON T. Cardiprin 1tab OD T. Isordil 10mg TDS S/L GTN 1tab PRN Now, please find the mistake in this list of drugs. |
|
|
|
|
|
Dec 17 2012, 05:37 PM
Return to original view | Post
#7
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(Syd G @ Dec 17 2012, 05:25 PM) Double dose aspirin? Cardiprin + Aspirin Good. Even someone who has just passed first year can pick up the error. The list of meds was prescribed by a junior MO who has just completed Housemanship. This MO is a graduate of an IPTA which is recognized by Singapore medical council. I really hope this is an "accidental" or "postcall" mistake. If not the rural folks are in big trouble. BTW, statin with fibrate is also not a good combination, as it can cause rhabdomyolysis. This combination is only used as second line therapy. This post has been edited by hypermax: Dec 17 2012, 05:40 PM |
|
|
Dec 17 2012, 06:44 PM
Return to original view | Post
#8
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(zstan @ Dec 17 2012, 06:24 PM) yeah but if the TGL levels are really high fibrates should be started along with statins. Monotherapy is always recommended as the initial therapy. If TG is > 5.7mmol/L at presentation, fibrate is started instead of statin. Combination therapy is only recommended if optimal monotherapy has failed to bring the lipid level down to target lipid goals after 8-12 weeks.Pls refer below pic for more info (from KKM guideline) 
This post has been edited by hypermax: Dec 17 2012, 06:45 PM |
|
|
Dec 17 2012, 08:23 PM
Return to original view | Post
#9
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(tqeh @ Dec 17 2012, 07:02 PM) It is likely that it is a unintentional mistake (for aspirin and ?cardiprin). As mentioned, I hope this is an unintentional mistake. If not then I am very worried about the quality of medical education.Not sure why gemfibrozil, does it actually really work? Definitely I wont feel comfortable starting them together. ? consider beta blocker in future? Statin is a must regardless of lipid studies given its role in secondary prevention. Plavix - did not state the duration? Was PCI done/ BMS/ DES? =D Such mistake would not be made if there is a pharmacist around checking discharge scripts? yes, agreed with the statin part. Statin should be started regardless of lipid profile post ACS/STEMI. Like you, I am also not comfortable with starting both fibrate and statin. if I am not mistaken, PCI is not routinely done for ACS. It is however, a gold standard for STEMI. Also, district hospital has no cardiologist, so PCI can't be done. Well, I am equally surprised that pharmacist didn't pick up the mistakes. QUOTE(zstan @ Dec 17 2012, 07:22 PM) yes but this was a discharge script. the patient might have already been started on initial therapy during admission. no? furthermore it is unclear on how long has the patient been admitted and what other drugs has the patient been taking along with his other test results. IMO besides the duplication of aspirin, its hard to justify whether the script is accurate or not based on present data. I guess you are confused a little. Let me clarify.gemfibrozil is to lower TGL levels, beta blockers work on the heart. both drugs work differently and have different mechanisms and different outcomes.  u only start statins if patient has a previous cardio/stroke event. if levels all ok then no issue la. but having said that if you get admitted probably got problem liao. u only start statins if patient has a previous cardio/stroke event. if levels all ok then no issue la. but having said that if you get admitted probably got problem liao.1. The guideline says optimal monotherapy before considering combination. Does 20mg of lovastatin or 300mg of gemfibrozil sound optimal to you? Are you aware of the max dosage for each drug? 2. Date of admission and discharge clearly written on the discharge note. Pls read it carefully. 3. All drugs taken by the patient are on the discharge note (usual practice for hospitals) 4. You dun only start statin post stroke or cardio event (where did you get this fact!?). Statin can be used in simple dyslipidemia as suggested by KKM guideline and guidelines all over the world. 5. tqeh is right on beta blocker for ACS. Beta blocker reduces the myocardial oxygen demand, thus it benefits patients with ACS/STEMI as well as CCF. I would suggest you do a read through of KKM's guidelines as well as books such as Sarawak Handbook of Medical Emergencies. Are you a doctor btw? If I am not mistaken, you are a pharmacist right? Added on December 17, 2012, 8:38 pm QUOTE(onelove89 @ Dec 17 2012, 07:40 PM) was looking for beta blockers in the chart and trying to make up what is what. to be honest i've never heard of cardiprin, we just say low dose asp 100mg. Cardiprin is combination of 100mg aspirin and 45mg glycine. It causes less gastrointestinal effect than conventional aspirin. but yeah, double prescription seems like an unintentional mistake? (overworked? still, not an excuse). I'll still put in statins and asp just for prevention, for high risk patients. as far as i know, statins are relatively safe, well, apart from some causing rhabdo, but chances are rather low. and I wouldn't be so sure on prescribing fibrates with statin tgt. This post has been edited by hypermax: Dec 17 2012, 08:38 PM |
|
|
Dec 17 2012, 08:55 PM
Return to original view | Post
#10
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(Syd G @ Dec 17 2012, 08:53 PM) Ah. Wanted to point out statin/fibrates combo but too unsure about that. Simply because lovastatin is the cheapest, and the only statin MO in KKM can prescribe (other statins need specialist prescription) Btw what's the reason for the MO to prescribe lovastatin instead of atorvastatin? Am more familiar with the latter since it's.....more famous price? dosage? compliance?This post has been edited by hypermax: Dec 17 2012, 08:56 PM |
|
|
Dec 17 2012, 09:07 PM
Return to original view | Post
#11
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(zstan @ Dec 17 2012, 08:55 PM) ah my bad then. didn't really check the DOA. so yeah, the fibrates shouldn't be prescribed together with statins. yeap the statin dose is quite low and not maxed out yet. my mistake on part 4. should be referring to high risk patients. For your info, some consultants even routinely prescribed statin for all type 2 diabetic patients above the age of 40 regardless of baseline lipid profile. |
|
|
Dec 17 2012, 09:26 PM
Return to original view | Post
#12
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(onelove89 @ Dec 17 2012, 09:13 PM) atorva should be more potent, rosuva too, compared to simva and lovastatin. but rosuva or crestor is very expensive. GH gave my mom lovastatin too. Maybe you should start taking statin then Lifestyle and exercise isn't doing much help for my cholesterol  been hovering above normal limits for a few years now. been hovering above normal limits for a few years now.  j/k j/k |
|
|
Dec 17 2012, 09:42 PM
Return to original view | Post
#13
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(tqeh @ Dec 17 2012, 09:36 PM) Yea, I think I know what are those drugs for after a few years of medical school. ACS refers to both unstable angina and NSTEMI, as both shares similar treatment plan. Plavix is usually continued for 6 weeks post ACS, and up to a year post PCI (dual antiplatelet therapy).I have not been studying in a while (like really super long) but correct me if I am wrong (I know there are a lot of senior doctors reading, please correct me if I am wrong!) I have no idea if gemfibrozil actually works in secondary prevention of cardiovascular event - I have not been taught about it, or read about it, or find out about it. Statins MUST be used in secondary prevention of cardiovascular event as Number Needed to Treat is low (?50, cant remember, depending on which studies you pick and which statin) Statins, can be used for primary prevention for high risk patient - oh well, nowadays ppl just treat numbers anyway lol even if they are perfectly healthy lol. NNT probably about 1000? pretty low yield. Perindopril has to be used post AMI as it reduces mortality (er, something to do with cardiac remodelling blabla) B-blocker, in patient post AMI without significantly impaired systolic function (Ie systolic heart failure), should be commenced on a B-blocker (low dose first, as tolerated) as it reduced recurrent AMIs and ?mortality. And yea, about the plavix part, I dont know man, I dont know whether the patient had a STEMI/NSTEMI. But the duration of plavix should be documented!!!!!!!!!!!!!!!!!! |
|
|
|
|
|
Dec 17 2012, 09:55 PM
Return to original view | Post
#14
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(tqeh @ Dec 17 2012, 09:42 PM) Is that from lecture / real life practice? I see so many cardiologists start people (private prac) on rosuvastatin. Hospital people tend to get atorva. Not really. Nowadays in hospitals we use more of lova and simva. Reason: cheaper This post has been edited by hypermax: Dec 17 2012, 09:55 PM |
|
|
Dec 17 2012, 10:38 PM
Return to original view | Post
#15
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(Syd G @ Dec 17 2012, 10:07 PM) Any comments on diuretics and beta-blockers? E.g why they're not given? U mean in the case of ACS? That's because in ACS the cardiac function is relatively well preserved, unlike in CCF. Thus diuretic is not needed to get rid of the extra fluid.Beta blocker should be given to patients with ACS, STEMI and CCF, as it reduces the myocardial oxygen demand. However, it should be introduced slowly as patients may complain of worsening of symptoms upon initiation of therapy. Also, beta blocke is contraindicated in COAD or Asthma patients. Like what zstan said, combination of diuretic and b blocker can cause new onset diabetes melitus. Thus close monitoring is required. |
|
|
Dec 17 2012, 10:45 PM
Return to original view | Post
#16
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(zstan @ Dec 17 2012, 10:02 PM) fibrates is more related to risk reduction in diabates compared to a cardiovascular event. its usage is more limited to reduce TGL levels and that's about it In diabetic patients, statin is still the first line therapy for risk reduction, unless TG>5.7 then fibrate will be used instead.plavix is there to prevent clot formation. working together with aspirin. from lectures  i would guess because its the most expensive.....? anyway, its just more incidence compared to other statins doesn't mean its bad otherwise it would be pulled out of the market. i would guess because its the most expensive.....? anyway, its just more incidence compared to other statins doesn't mean its bad otherwise it would be pulled out of the market. Btw, the mechanisms for both aspirin and clopidogrel are important for MRCP part 1. One has to know them by heart if keen for MRCP. This post has been edited by hypermax: Dec 17 2012, 10:52 PM |
|
|
Dec 18 2012, 09:47 AM
Return to original view | Post
#17
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(D_s_X @ Dec 18 2012, 09:10 AM) TBH I haven't seen much use of fibrates (none that I can recall, for that matter) so far. Don't know if it has fallen out of favour in Australia (Hobart) or it's just that I've been not looking close enough. B blocker is contraindicated in both coad and asthma as it causes bronchial constriction. I have not seen patients with coad or asthma being started on b blocker. Perhaps the patients u have seen are having cardiac asthma?P/S: B-blockers can mask the adrenegic symptoms of hypoglycaemia as well (!use in high risk patients). Hypermax, are b-blockers and absolute contraindication in COPD and Asthma? I ask this only because I have seen patients on them, where the doctors say, B-blockers work for them. |
|
|
Dec 18 2012, 10:03 AM
Return to original view | Post
#18
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(Syd G @ Dec 18 2012, 09:55 AM) In theory, that only applies to non-selective BBs right? How atenolol? The cardio selective bb loses its receptor selectivity at higher dosage.http://en.m.wikipedia.org/wiki/Beta_blocker Read under the section adverse effects. This post has been edited by hypermax: Dec 18 2012, 10:11 AM |
|
|
Dec 18 2012, 05:34 PM
Return to original view | Post
#19
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
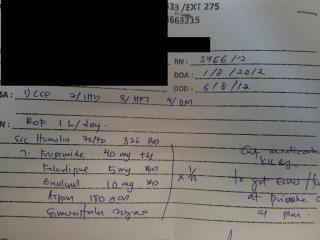
OK, again. Pls spot the mistake in this discharge note.
|
|
|
Dec 18 2012, 11:38 PM
Return to original view | Post
#20
|
|
Senior Member
2,524 posts Joined: Jan 2003 From: Beneath the starry night |
QUOTE(zstan @ Dec 18 2012, 10:23 PM) Last one is simvastatin. ccb given with ccf? Wanna kill the patient mer Good one. The list of meds were prescribed by a senior MO graduated from a renown university in developed country. From the same hospital as the previous case. That's why I am against judging a doctor purely based on where he graduated from. Added on December 18, 2012, 11:40 pm QUOTE(Syd G @ Dec 18 2012, 06:30 PM) Can only read Humulin, Furosemide, Felodipine....maybe Enalapril, Aspirin and ... not so sure about the last one. Furosemide is needed in this case as the patient has CCF. This is again a case of benefits outweigh the risks.Patient given diuretics despite being DM n on insulin treatment? This post has been edited by hypermax: Dec 18 2012, 11:40 PM |
| Change to: |  0.0235sec 0.0235sec
 0.42 0.42
 7 queries 7 queries
 GZIP Disabled GZIP Disabled
Time is now: 5th December 2025 - 09:22 PM |
 Quote
Quote